WHO Deletes Misleading Tweet That Spread Paranoia About COVID-19 Reinfection

By Robby Soave
This weekend the World Health Organization (WHO) had to delete a misleading tweet about the coronavirus. Unfortunately, several media outlets had already cited it, spreading unwarranted fear about the likelihood of secondary COVID-19 infections.
On Friday, the WHO published a scientific brief on “immunity passports“—the idea that governments should grant special documents to citizens who test positive for COVID-19 antibodies, allowing them to move about freely. The WHO warned that this is premature, since “no study has evaluated whether the presence of antibodies to SARS-CoV-2 confers immunity to subsequent infection by this virus in humans.”
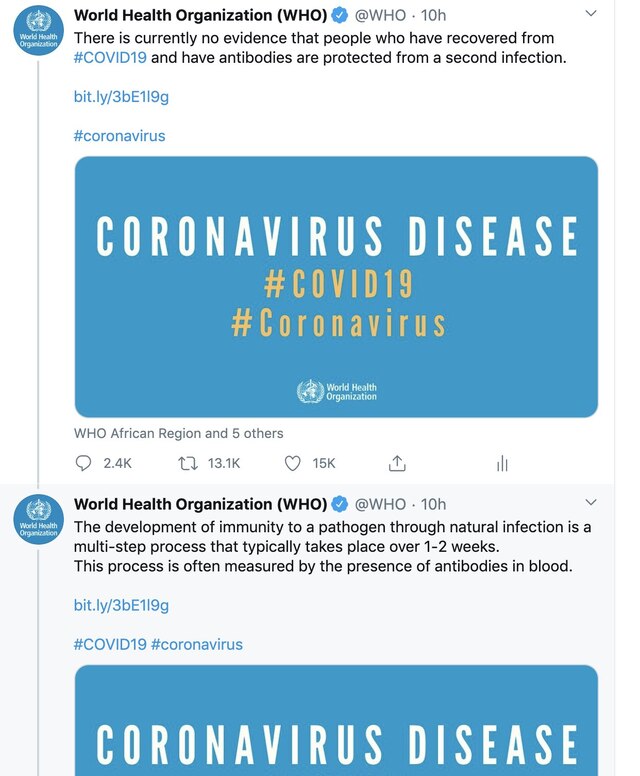
The WHO is correct that scientists have not determined the degree of immunity enjoyed by COVID-19 survivors. But the tweet version of the brief was missing important context, and it said only this: “There is currently no evidence that people who have recovered from #COVID19 and have antibodies are protected from a second infection.”
That’s technically true: There’s no evidence of immunity. But that’s because COVID-19 is new and the matter hasn’t been conclusively studied yet. Scientists have good reason to expect COVID-19 survivors to have some immunity to the virus, though they’re unsure how strong it will be or how long it will last.
“When they say ‘no evidence’ they mean something like ‘no definitive proof, yet,'” wrote statistician Nate Silver in response to the WHO tweet. “But the average person is going to read it as ‘there’s no immunity to coronavirus,’ which is likely false and not a good summation of the evidence.”
Indeed, Bloomberg News reported this story with the headline “WHO Warns You May Catch Coronavirus More Than Once.” Here’s how the article started:
Catching Covid-19 once may not protect you from getting it again, according to the World Health Organization, a finding that could jeopardize efforts to allow people to return to work after recovering from the virus.
That’s just wrong. There is no “finding” to speak of here, just an absence of definitive proof that antibodies confer a degree of immunity. Many readers undoubtedly would come away from these statements with a level of anxiety—You can get it again! We’re doomed!—that isn’t merited.
The WHO ultimately conceded that its declarations about immunity passports were overly pessimistic and deleted the tweet in question.
From parroting the Chinese communist government’s lies about COVID-19 to wrongly warning people against wearing masks, the WHO has badly mishandled its communications about the pandemic. The organization really needs to get its act together.
It’s Not Fake News: Trump Did Actually Suggest That Injecting Bleach Could Be a Cure for COVID-19

By Jacob Sullum
This morning Kayleigh McEnany, the new White House press secretary, slammed news outlets for reporting that President Donald Trump had suggested injecting household disinfectants might prove to be an effective cure for COVID-19. “President Trump has repeatedly said that Americans should consult with medical doctors regarding coronavirus treatment, a point that he emphasized again during yesterday’s briefing,” she said. “Leave it to the media to irresponsibly take President Trump out of context and run with negative headlines.”
Is that what they did? The context of Trump’s remarks was a presentation by William Bryan, a senior Department of Homeland Security official who oversees science and technology issues. Bryan summarized the results of experiments that found exposure to sunlight dramatically reduced the half-life of coronavirus particles on nonporous surfaces such as door handles and stainless steel. He also noted that applying bleach “will kill the virus in five minutes,” while isopropyl alcohol “will kill the virus in 30 seconds.” Here is Trump’s response to that information, according to the official White House transcript of the press briefing:
I asked Bill a question that probably some of you are thinking of, if you’re totally into that world, which I find to be very interesting. So, supposing we hit the body with a tremendous—whether it’s ultraviolet or just very powerful light—and I think you said that that hasn’t been checked, but you’re going to test it. And then I said, supposing you brought the light inside the body, which you can do either through the skin or in some other way, and I think you said you’re going to test that too. It sounds interesting…
And then I see the disinfectant, where it knocks it out in a minute. One minute. And is there a way we can do something like that, by injection inside or almost a cleaning. Because you see it gets in the lungs and it does a tremendous number on the lungs. So it would be interesting to check that. So, that, you’re going to have to use medical doctors with. But it sounds—it sounds interesting to me.
Trump’s comments apparently were alarming enough to prompt an advisory from Reckitt Benckiser, the British manufacturer of Lysol and Dettol cleaning products. I say “apparently” because the advisory does not mention Trump specifically, but it was first posted around noon London time, about 12 hours after the press briefing, which concluded close to midnight for the folks at Reckitt Benckiser. Here is what they said:
Due to recent speculation and social media activity, RB (the makers of Lysol and Dettol) has been asked whether internal administration of disinfectants may be appropriate for investigation or use as a treatment for coronavirus (SARS-CoV-2).
As a global leader in health and hygiene products, we must be clear that under no circumstance should our disinfectant products be administered into the human body (through injection, ingestion or any other route). As with all products, our disinfectant and hygiene products should only be used as intended and in line with usage guidelines. Please read the label and safety information.
Did the president recommend that Americans inject themselves with bleach as a COVID-19 cure or prophylactic? Strictly speaking, no. As McEnany emphasized, he said “you’re going to have to use medical doctors” for that sort of thing. But he did idly speculate that, since disinfectants kill the COVID-19 virus on surfaces, it was worth investigating whether they might work as a treatment, and he specifically mentioned “injection,” which was not only scientifically naive but reckless given the prevalence of quack remedies and wacky ideas about how to ward off the disease.
Unlike Trump’s hopeful remarks about the anti-malarial drug hydroxychloroquine as a COVID-19 treatment, which people unfairly blamed for the death of a man who swallowed the fish tank cleaner chloroquine phosphate, his out-loud wondering about the possible benefits of injecting disinfectant had no scientific basis and might encourage potentially deadly experimentation. “This notion of injecting or ingesting any type of cleansing product into the body is irresponsible, and it’s dangerous,” pulmonologist Vin Gupta told NBC News. “It’s a common method that people utilize when they want to kill themselves.”
Trump’s suggestion about using “ultraviolet or just very powerful light” to eliminate the virus inside infected patients, while less likely to kill anyone, was equally fanciful (although it did work on the flying jellyfish that attacked Mr. Spock, albeit with a major side effect). “I would like you to speak to the medical doctors to see if there’s any way that you can apply light and heat to cure,” he told a reporter. Turning to Deborah Birx, the physician who runs the White House’s coronavirus task force, he asked, “Deborah, have you ever heard of that? The heat and the light…relative to this virus?” Her answer was firm but diplomatic: “Not as a treatment.”
Update: Today Trump claimed he was just kidding about injecting disinfectants, an explanation that was notably absent from McEnany’s statement. “I was asking a question sarcastically to reporters like you just to see what would happen,” he saidduring a bill signing. You be the judge:
More Evidence That Hydroxychloroquine Is Not a COVID-19 Silver Bullet

By Ronald Bailey
Some small preliminary studies published a month ago suggested that the anti-malarial drugs chloroquine and hydroxychloroquine, in combination with the antibiotic azithromycin, might be a potent treatment for COVID-19. Subsequently, at a March 19 press conference, President Trump touted chloroquine, an analog of hydroxychloroquine, as a treatment for COVID-19. “It’s shown very encouraging, very, very encouraging early results, and we’re going to be able to make that drug available almost immediately, and that’s where the FDA has been so great,” said the president.
Obviously, it would be tremendously good news if chloroquine and hydroxychloroquine turn out to be really effective in treating COVID-19. Unfortunately, more recent research is not validating that hope.
A new nationwide retrospective study of patients treated at Veterans Administration medical centers is providing the largest dataset yet reported on the outcomes of COVID-19 patients treated with hydroxychloroquine, with or without azithromycin, anywhere in the world. The results are unfortunately not promising.
“Hydroxychloroquine use with or without co-administration of azithromycin did not improve mortality or reduce the need for mechanical ventilation in hospitalized patients,” reported the researchers, who are affiliated with the Universities of Virginia and South Carolina. “On the contrary,” they added, “hydroxychloroquine use alone was associated with an increased risk of mortality compared to standard care alone.”
The fact that this is an observational study rather than a randomized controlled trial is an important caveat with respect to evaluating its conclusions. The study assessed 368 male patients treated for COVID-19 at Veterans Health Administration medical centers. In the study, 97 patients were treated with hydroxychloroquine (HC), another 113 received hydroxychloroquine in combination with the antibiotic azithromycin (HC+AZ), and 158 were not treated with hydroxychloroquine (no HC), receiving standard supportive management.
The researchers reported that “there were 27 deaths (27.8%) in the HC group, 25 deaths (22.1%) in the HC+AZ group, and 18 deaths (11.4%) in the no HC group. Mechanical ventilation occurred in 13.3% of the HC group, 6.9% of the HC+AZ group, and 14.1% of the no HC group.” In other words, the patients not treated with hydroxychloroquine (No HC) had the lowest rate of death compared to the HC and HC+AZ cohorts. It is worth noting that the HC + AZ group were less likely to require mechanical ventilation.
President Trump, when asked about the disappointing results of the Veterans Administration study, replied, “I don’t know of the report. Obviously, there have been some very good reports, and perhaps this one is not a good report. But we’ll be looking at it.”
In the meantime, new treatment guidelines issued by an expert panel convened by the National Institute of Allergy and Infectious Diseases recommended against the use of the combination of hydroxychloroquine plus azithromycin because of the potential for toxicities. The panel also observed that there “are insufficient clinical data to recommend either for or against using chloroquine or hydroxychloroquine for the treatment of COVID-19.” If physicians choose to use either of the two antimalarials, the panel recommends that they should carefully monitor patients for dangerous heart rhythms problems known to be associated with the two drugs.
The researchers who analyzed the efficacy of hydroxychloroquine in treating Veterans Administration patients conclude, “These findings highlight the importance of awaiting the results of ongoing prospective, randomized, controlled studies before widespread adoption of these drugs.”
While further research may eventually show that these drugs could offer some therapeutic benefits, they are right now not looking like the anti-COVID-19 silver bullets many people had hoped they would be.
Fox News is Wrong: COVID-19 has Killed Many More People Than Reported
Bureau of Prisons Reverses Coronavirus Home Confinement Policy
By C.J. Ciaramella
The Bureau of Prisons (BOP) abruptly changed its policy yesterday for which inmates are eligible for early release into home confinement because of the threat of COVID-19, advocates and family members of inmates say, crushing the hopes of some inmates who had already been moved into pre-release quarantine.
According to multiple accounts from family members and the criminal justice advocacy group FAMM, the BOP informed inmates on Monday that it would not be waiving a requirement that inmates serve 50 percent of their sentence before they can become eligible for home confinement, despite earlier indications that it would.
It’s unclear how many inmates who were approved for early release were disqualified.
The BOP did not immediately respond to a request for comment.
“The BOP is playing with people’s lives,” Kevin Ring, president of FAMM, said in a statement. “It’s nothing short of cruel to tell hundreds of people they are going home, notifying their families and quarantining them for days, only to change your mind afterward.”
Attorney General William Barr issued a directive on March 26 expanding compassionate release and home confinement transfers of elderly and at-risk inmates to mitigate potentially deadly COVID-19 outbreaks. Politico reported on April 9 that the BOP quietly expanded the directive and waived the 50 percent requirement as the virus spread through several federal prisons.
Inmates who are approved for early release are put into quarantine for two weeks. However, Ring tweeted yesterday that family members of inmates traveled to FCC Coleman, a federal prison complex in Florida, expecting to pick up their incarcerated loved ones, only to be told the policy had been changed.
Reason received a message yesterday from a family member of a man incarcerated at FCI Elkton, a federal prison in Ohio that has been hit particularly hard by the virus.
“Last week, my Dad was told that he would be going to home confinement based on AG Barr’s memo,” the family member wrote. “They made him sign numerous documents on multiple occasions. Today, they told him that he was denied for home confinement because he hasn’t served 50% of his sentence yet. The 50% threshold is explicitly NOT a criteria, yet they have still done this to him. Not to mention the sentence in the first place is way above the guidelines. What they are doing to people is cruel and unusual. It isn’t right.”
Politico received a similar email:
“They just posted a new BOP Bulletin a few minutes ago, reversing the Barr decision and requiring that those released to home confinement must have served 50% of their sentence,” Stephen Donaldson, son of an inmate at a prison in Georgia, wrote in an email to POLITICO. “I was hoping to have my father home. He tells me a number of other inmates had started the quarantine pre release and then were told of the reversal.”
The notifications appear to have gone out throughout the federal prison system:
Yesterday Judge Alison Nathan of the U.S. District Court for the Southern District of New York called the BOP’s quarantine policies “illogical” and “Kafkaesque” and said they put inmates at greater risk of contracting COVID-19.
According to the BOP’s most recent numbers, there are 497 federal inmates and 319 staff infected with the virus. So far, 22 inmates have died from COVID-19 complications. There are roughly 20,000 federal inmates over the age of 55.
FAMM sent a letter today to BOP Director Michael Caraval today requesting more information and transparency from the agency.
“Tens of thousands of families across the country are deeply and understandably frightened for the health and safety of their incarcerated loved ones,” Ring wrote. “The people inside BOP’s facilities are confused, frightened, and vulnerable. They deserve maximum transparency from the BOP.”
What Each Side of the COVID-19 Debate Should Understand About the Other

By Brian Doherty
Beyond its devastating effect on the health of hundreds of thousands and the livelihood of millions, the COVID-19 crisis is a harshly vivid example of Americans’ inability to understand, fruitfully communicate with, or show a hint of respect for those seen to be on other side of an ideological line.
Americans are divided about the best way to proceed from here, three months since the first case was diagnosed in the U.S. The division is more vivid and harsh on social networks than in the polls, where a vast majority of Americans still think strong lockdowns are the best idea moving forward. Such Americans think the economy needs to stay shut down by law until a vaccine or some effective treatment is developed that ensures no more, or a very tiny number of, people will be seriously harmed or killed by COVID-19.
On the other hand, some Americans think, on balance, the country’s overall quality of life demands we start letting people and businesses make their own decisions about whether it is safe to go out in public or conduct business openly, especially given access to simple prophylactic measures such as gloves and masks.
To sum up each side in the language of their angriest opponents: The “Closers” want to demolish nearly all Americans’ ability to live, and destroy nearly all the wealth our society has built up over decades, by halting the wheels of most commerce for the forseeable future. And the “Openers” are so dedicated to keeping GDP growing and so ignorant of science they want to see hundreds of thousands, maybe millions, of Americans die of a hideous disease because they don’t understand how contagion works.
Both Closers and Openers, though, have a combination of reasons, theories, guesses, and value judgments of a sort many sane people have always made, that make their respective positions make sense to them. Neither side should be blithely written off as either idiotic or sinister or not thinking, in their own way, of human well-being.
The Openers think they see many costs the Closers are not adequately considering, and wonder if the long-term benefits of closing are smaller than the Closers believe.
Openers are worried about over 15 million Americans out of work, and look at industries including hospitality, food service, entertainment not beamed in via smart TVs, sports, construction, oil, education, law, and even, counterintuitively, medical care (not to mention all non-food retail and any financial or other entities who depend on rents and mortgages continuing to be paid in the months to come) all either destroyed or seriously weakened and unable to move forward at anything near their old strength.
They worry that the web of commerce is so complicated and hard to build or to gently snip off portions of that as-yet-unrealized problems will arise with an economy that acts as if making, transporting, and selling food will keep working fine even if nothing else is.
Openers see the government’s short-term solution of loans and giveaways both personal and corporate in the trillions and growing as seriously dangerous, with a real possibility of upending our fiscal and monetary systems under debt and/or money supply explosions that could become truly unsustainable and take decades to recover from. They see states and localities facing already near-impossible pension and other obligations and shrinking tax bases pushed closer, faster, to an abyss of complete inability to function, with dire effects on citizens.
Openers think it is worth seriously wondering about many as-yet-unknown facts, such as actual current infection rates, asymptomatic numbers vs. ill numbers, and death rates and age distributions of same. They understand that the Openers vs. Closers debate involves cost/benefit decisions, and they want to understand the benefits as well as possible. Openers do believe that one cannot build public policy as if “saving one life” (or, more accurately, delaying one death) is the sole goal and think it important to note that in no other situation and with no other illness have we acted as if that was a reasonable goal.
Openers do take very seriously the idea of “flattening the curve“—perhaps, an Opener might think, even more seriously than the Closers do, because Openers can’t help but think that this virus will, over whatever length of time, infect everyone everywhere until herd immunity is reached or by whatever method R0 becomes less than one.
That is, Openers think it reasonable to consider that we are not facing a choice to “save lives” (or delay deaths) in the sense of preventing infections from ever occurring, which is more or less impossible now. The only really important consideration now is excess deaths or serious illness complications caused by inadequate medical facilities because at some given day in some specific hospital COVID cases are overwhelmingly large.
Openers thus wonder why more public policy decisions aren’t being made based on a rigorous calculation of that number, now and in a reasonably foreseeable future based on best understanding of our hospital capacity, how quickly we could increase that capacity if that became public policy priority one, and the prevalence, percentage symptomatic, and percentage brought to brink of death by the disease. Openers tend to believe a “testing” solution or a “vaccine” solution are both outside the realm of plausibility now and for any foreseeable future.
The Closers, meanwhile, are seen by hostile Openers as driven by some sinister desire for a scenario in which the only “reasonable” endgame for living anything like a free life is either or both enforced vaccination and constant registered surveillance, or who for partisan political reasons want to make 2020 so miserable in America that Trump will lose the election.
However, the Closers have many reasons that make sense to them to keep things closed that don’t involve a mad desire to tyrannize the country or harm Trump. Closers see and acknowledge the economic damage we are suffering, but they see most of that damage already inherent in the unchecked spread of a disease that kills or seriously harms people to a greater extent than any we’ve dealt with in a century. They thus don’t see the economic problems as solvable just by “opening up America.”
Closers see anyone who, aware that COVID-19 exists and can spread asymptomatically, then does anything that could in any way risk someone else catching it as morally akin to murderers. The Closers are very concerned with the fact that people are dying from this disease, in the tens of thousands—that COVID-19 is indeed after just three months by best available data likely killing nearly double as many Americans as were killed by the flu this flu season. Closers thus consider some Openers’ niggling obsessions about marginal accuracy in that fatality count as irrelevant to any policy decision we are now facing. Even if those numbers are not 100 percent accurate, they are large enough to make worrying over their precise size peculiarly beside the point.
Closers also recognize that the death count is not the best or most accurate way to assess the threat COVID-19 presents and thus what sacrifices are reasonable or prudent to try to keep it from spreading faster. The disease is known or suspected to be neurotoxic and hepatoxic, not merely a respiratory illness, and might cause serious and possibly long term damage to the heart, blood, liver, and nervous systems of those who contract, it even if they “recover.”
Closers are also sure that we can’t know how much damage COVID-19 will eventually cause in our nation just based on the experience of the past 6 weeks, when we have been doing our best to keep people from getting close enough to each other in large enough numbers to truly and quickly unleash COVID-19. Thus to the Closers, any calculations based on “existing data” that are supposed to settle the question of whether we’ve done enough, or even too much, and can now “open up” are beside the point, in a genuinely dangerous way. If it’s not an intolerable nightmare yet, they would say, that’s because we are staying shut down.
The damage done by the disease and/or the policy reaction to the disease is baked into our nation, and will almost certainly echo strongly through at least the rest of this decade. Our nation might be slightly better off, though, if more of us did not compound that civic damage through a ferocious and unmanageable cultural and political squabble based on refusing to consider the reasons the other side thinks what they do with anything approaching intellectual charity and empathy.
We could, though might not ever, know the answer to every currently unanswered question about the disease’s spread, extent, and damage. We might figure out accurately the long term damage to life and prosperity the economic shutdown is causing. Even if or when we do, though, human beings of goodwill and intelligence might come to a different value judgment about what policy is best overall. Because we all have to make those tricky, very hard-to-discuss-dispassionately decisions (of a sort we have always made every day on the margins without explicit debate) about when we think it best to stop shaping policy toward the sole goal of extending every possible life. The answer either side might come to need not be condemned as based in idiotic recklessness or tyrannical fantasies.
Snorkel Respirators, 3D-Printed Masks, and Other Grassroots Efforts To Fight COVID-19
A Harvard Plan To Use Massive COVID-19 Testing To Reopen the Economy
By Ronald Bailey
To fully restart the U.S. economy by August, massive population testing for infections with the virus that causes COVID-19 is essential, according to the roadmap to pandemic resilience just issued today by the Safra Center for Ethics at Harvard University. Testing results should be available the next day at the latest. The roadmap also sketches out a system of tracing the contacts of people who are infected by the coronavirus. Those contacts are warned about their exposure and tested numerous times. If a contact’s tests turn positive they should be provided supported isolation that includes job protections, safe shelter, food, and health care. The authors of the report estimate that this scheme for testing, tracing, and supported isolation (TTSI) would cost between $50 to $300 billion over two years. As they note this is extremely cheap compared to “the economic cost of continued collective quarantine of $100 to 350 billion a month.”
How much testing would be required to implement their proposed roadmap? “We estimate that steady-state testing levels that would permit replacing collective stay-at-home orders as the main tool for disease control with a testing—tracing-and-warning—supported-isolation, or TTSI, methodology will eventually need to reach a capacity to test 2 to 6% of the population per day, or between 5 and 20 million people per day,” note the authors.
How would they achieve a rapid increase in testing capacity? Given how badly federal agencies botched testing as the coronavirus outbreak was growing, the authors wisely recommend turning to the private sector. “The government should not hesitate to pay substantial sums to incentivize the private sector to apply ingenuity and speed to develop solutions,” note the authors. “Prizes and advance market commitments are two tools to be considered.”
In order to warn people who have come into contact with an infected person that they should be tested, the authors recommend initially hiring and training 100,000 contact tracers at a cost of $3.6 billion. Such manual contact tracing could be supplemented with opt-in peer-to-peer cell phone warning apps. The researchers suggest that the deployment of such apps include maximal privacy protection, use open-source code amenable to independent and regulatory audit, and prohibit the use of any data from these apps for commercial purposes.
Frustratingly, the Safra Center authors do not discuss prohibiting government abuse of the tracking functions and data collected by the apps (that is, immigration authorities and law enforcement). In order to forestall our government from using the pandemic as an excuse to further violate our civil rights and privacy, we should adopt the proposals recommended by the Ada Lovelace Institute (ALI) in its similar testing-and-tracking scheme for the United Kingdom. The ALI authors warn that “there is a real risk that the expansion of state intrusion into individuals’ lives that occurs during emergencies endures beyond the originating crisis.” Consequently, they recommend:
Legal and technical sunset clauses must be built into the design of new powers and technologies. Government must provide advance primary legislation regulating the processing of data by both public and private sector actors in the use of technology to transition from the crisis. Government must encourage privacy-by-design in technical implementations and must choose privacy-preserving protocols to underscore technical measures.
Recommendations like these must be part of any wide-scale U.S. COVID-19 testing and tracing plan.
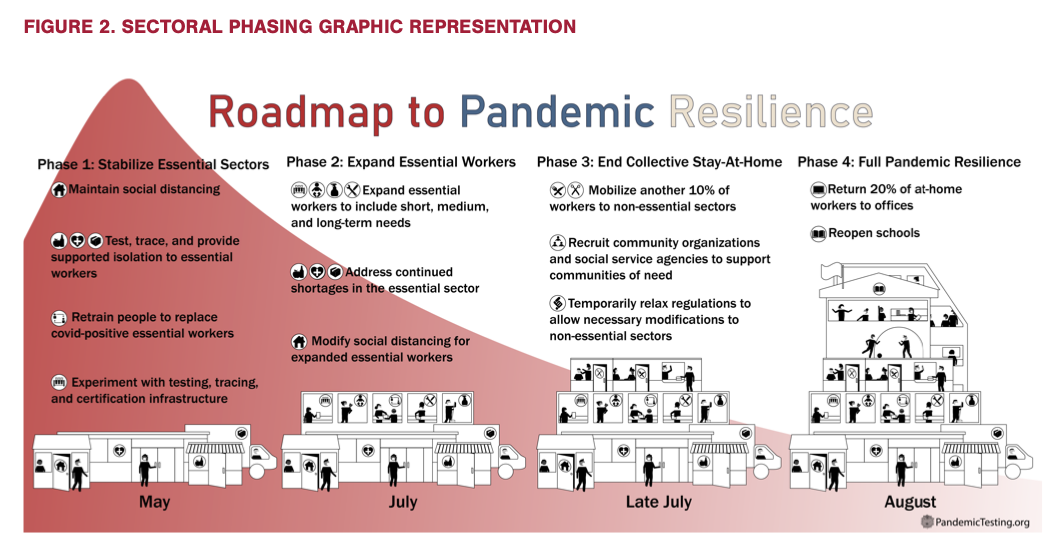
The Safra Center authors sketch out a four-phase program aimed at fully reopening the economy by the end of this summer. During phase one, they recommend increasing publicly-funded diagnostic testing capability to 2 million tests per day, focusing on everyone with symptoms and their close contacts, as well as essential workers, nursing home residents, and incarcerated people. With this amount of testing, they estimate that 40 to 55 percent of people could return to work.Safra Center
With the testing and tracing regime solidly in place, COVID-19 case rates would decline, thus enabling the initiation of phase two in the next month. With further expansion of testing and tracing, 70 percent of the workforce could return to work. Those who can work at home would still do so and vulnerable people (e.g. those over age 60) would continue to limit their time in the community. In phase three, increased testing and tracing that covers 80 percent of the workforce in localities would allow most non-telecommuting laborers to return to work. In phase four, universal testing would be available and schools could reopen.
The roadmap, as outlined, could likely work. However, assuming that the real and substantial technical difficulties in ramping up that much daily testing can be overcome, the ongoing economic distress makes it unlikely that the public would endure the implementation of such a careful plan. And even if the public did remain patient, it’s doubtful that the bureaucrats and politicians in Washington, including our chaotic president, have the competence to pull it off.
Despite COVID-19 Lockdowns, Licensed Marijuana Sales Continue in the Vast Majority of States With Legal Pot

By Jacob Sullum
Measured by marijuana sales, 4/20 came early this year as cannabis consumers scrambled to stock up, apparently worried that COVID-19 lockdowns might cut off their legal supply. After local governments in the San Francisco Bay Area imposed stay-at-home orders in March, The New York Times reports, sales of edibles “surged to levels typically only seen around April 20, or ‘4/20,’ the annual, if unofficial, marijuana appreciation holiday.”
That initial panic, which the chief executive of a medical dispensary in Pennsylvania likened to “hoarding toilet paper,” seems to have subsided now that the legal status of marijuana sales under state and local lockdowns has been clarified. The vast majority of states where cannabis is legal have deemed marijuana merchants “essential,” meaning they are exempt from business closure orders, although new restrictions may apply.
According to a tally by Marijuana Business Daily, medical dispensaries are exempt from business closure orders in 28 of the 33 states that allow patients to use cannabis for symptom relief. Of the 10 states that have legalized recreational sales, eight are allowing them to continue. Licensed recreational stores have not opened yet in Maine, although it has been four years since voters approved them. Only Massachusetts has closed recreational outlets while allowing medical sales to continue.
Here is a summary of the rules for marijuana merchants in states that have legalized recreational sales:
Alaska
Recreational and medical marijuana retailers remain open, subject to social distancing rules. The cannabis industry is urging the state to legalize curbside pickup.
California
The Bureau of Cannabis Control notes that Gov. Gavin Newsom’s March 19 business closure order “identifies certain services as essential, including food, prescriptions, and healthcare.” And “because cannabis is an essential medicine for many residents, licensees may continue to operate at this time so long as their operations comply with local rules and regulations.”
Colorado
Gov. Jared Polis is temporarily allowing online sales of marijuana, which means “both Medical and Retail Marijuana Stores may accept and complete online and telephone sales transactions.” Colorado’s Marijuana Enforcement Division is allowing curbside pickup, as long as it is consistent with local regulations and the transactions occur on private property, as well as sales from drive-through or walk-up windows.
Illinois
Gov. J.B. Pritzker’s March 21 business closure order classifies “licensed medical and adult use cannabis dispensaries” as essential. Like other exempt retailers, they have to follow social distancing rules.
Maine
Although a 2016 ballot initiative legalized recreational use, licensed sales to recreational consumers have not begun yet. Dispensaries serving state-approved patients have been classified as essential “medical facilities.” Various precautions apply to in-store sales.
Massachusetts
Gov. Charlie Baker is allowing sales to registered patients but has ordered recreational stores to close. “Licensed medical marijuana retailers” are exempt from Baker’s March 23 business closure order because they provide essential “health care services.” Recreational retailers did not make the cut, although liquor stores did, under the heading of “food and agriculture.”
Michigan
Gov. Gretchen Whitmer, who has banned sales of vegetable seeds, paint, and other products she deems nonessential, is nevertheless allowing medical and recreational marijuana sales to continue. Michigan’s Marijuana Regulatory Agency is temporarily allowing home delivery and “encourages” consumers to use that option “when applicable.” Regulators are also temporarily allowing curbside pickup.
Nevada
The Department of Taxation says “licensed cannabis stores and medical dispensaries will remain open but must adhere to strict social distancing protocol during this time.” That means “licensees must not allow individuals to congregate in stores or outside while waiting”; “patient consultations should be limited to phone or video only”; and “consumers are strongly encouraged to utilize delivery services when applicable, or complete orders online or over the phone.”
Oregon
The Liquor Control Commission, which also regulates marijuana sales, is temporarily allowing curbside delivery of cannabis products. In-store sales are also permitted. The commission has increased the daily limit from eight to 24 ounces for medical marijuana buyers.
Washington
The Liquor and Cannabis Board says “cannabis producers, processors, retailers and approved labs are considered essential and not required to close due to the coronavirus restrictions.” To facilitate social distancing, the board is allowing recreational consumers as well as patients to use curbside pickup. General retailing restrictions, such as keeping customers at least 6 feet apart, apply to in-store sales.
The Times says the exemptions for marijuana merchants constitute “official recognition that for some Americans, cannabis is as necessary as milk and bread.” Except in Massachusetts, where it is not even as necessary as booze.

{kind=link}